How to Support a Baby Detoxing From Opiod
Neonatal Abstinence Syndrome
There are many variables that impact if, how, and when an infant will experience withdrawal symptoms. These include:
- timing of the mother's well-nigh recent intake of opioid
- maternal metabolism
- placental metabolism
- infant metabolism and excretion
- maternal taking of other substances, including cigarettes, cocaine, hypnotics sedatives, and/or barbiturates[1]
Opioid withdrawal in a newborn causes central nervous organization excitability or hyperirritability, such as tremors, potent or rigid muscle tone, and vasomotor signs, as well as gastrointestinal signs, including vomiting and loose stools. The onset of the symptoms varies; withal, infants exposed to heroin or other short-acting opioids volition typically prove symptoms within the first 48–72 hours later on birth. Those exposed to methadone or buprenorphine, which are longer acting opioids, will oft present symptoms later than 72 hours, merely unremarkably inside the outset four days. The severity and elapsing of the withdrawal symptoms can be influenced by exposure to other substances, including tobacco and barbiturates.[1] Poly-substance use may be more the rule for women with an opioid-use disorder, with 2 notable exceptions: (a) women who are in long-term recovery and receiving medication-assisted treatment (who go pregnant after beginning handling), and (b) women whose opioid utilize was limited to prescribed opioids taken nether medical supervision for hurting management.
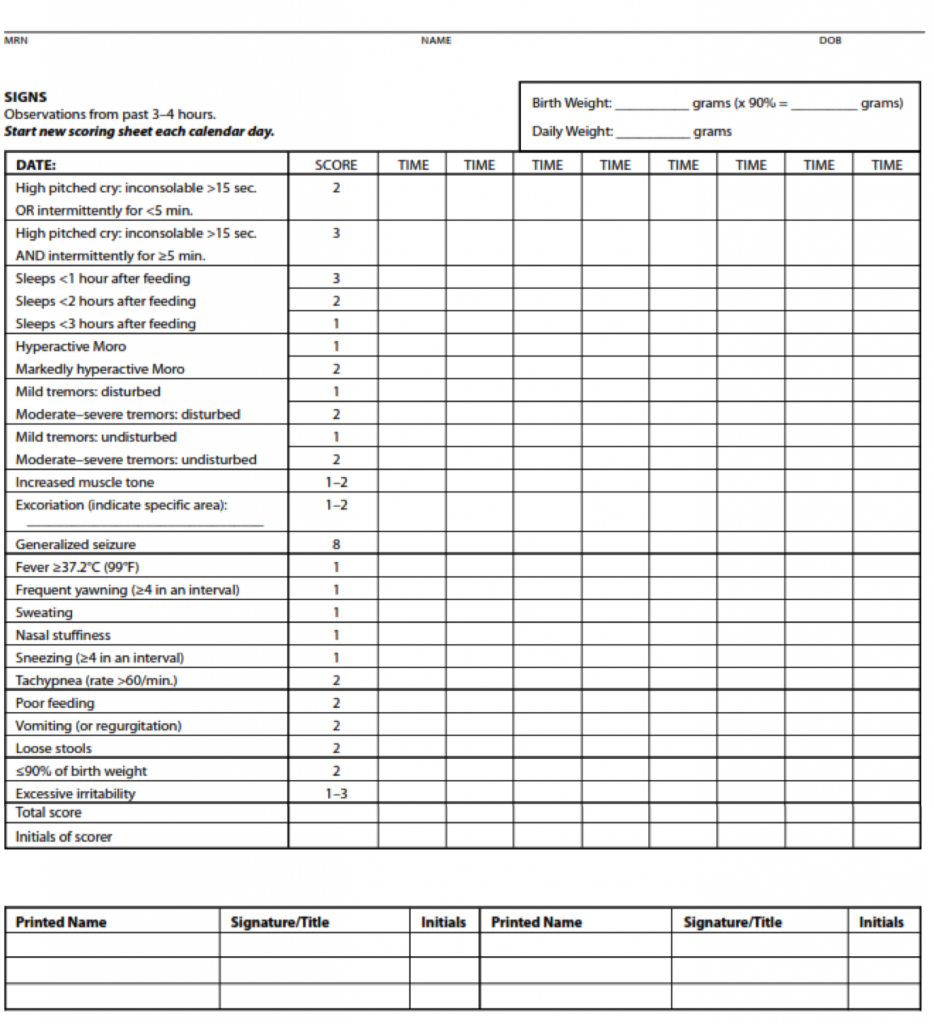
To appraise the signs and severity of withdrawal in an babe, practitioners use a standardized scoring system such as the system first adult by Finnegan[ii] and later on modified by Jansson[3] and others. When this type of standardized scoring tool is used by well-trained healthcare professionals, the instrument enables the practitioner to make an cess, identify the withdrawal symptoms, document the infant'south withdrawal, and initiate the appropriate handling regimen, when needed.[4] Increasingly, practitioners are education the mothers how to utilise the scoring tool, allowing the mother to actively participate in her infant'south monitoring. Elevated scores signal a clinically significant withdrawal, and the infant might be a candidate for pharmacologic treatment.
At times, substance exposure is identified using toxicology screening of the newborn'southward urine and meconium (i.due east., first stool), peculiarly in cases in which the mother has not been in a substance-use disorder treatment program and has not been forthcoming with the medical team. Urine testing (i.due east., urinalysis) generally reflects substance exposure within the past several days, depending upon the substance. Results of these tests are quickly available; all the same, urinalysis produces a high charge per unit of fake–negative results due to the rapid clearance of most drugs from the newborn's system and the difficulty in obtaining the book of urine need for testing from an infant in the first day of life. Meconium toxicology screens can reveal substance exposure during the previous several months of pregnancy. However, obtaining the meconium test results may take several days, by which time the mother and babe are probable to have been discharged. Umbilical string tissue is another diagnostic for infant toxicology. One advantage of umbilical cord tissue sampling is that the string is always available, where meconium can be missed due to excretion in utero. The results are available faster, which allows for better informed treatment and going home decisions. The examination requires half dozen inches of umbilical cord tissue and provides a longer histology of prenatal drug exposure, just may also detect medications used in labor and commitment.
Opioid withdrawal symptoms can mirror symptoms of other conditions in a newborn, such every bit infections, very depression blood saccharide, very depression blood calcium, low thyroid hormone, and issues with the brain (e.one thousand., cognitive palsy).[1]
Neonatal Forbearance Syndrome (NAS) Scoring and Direction
The Finnegan Neonatal Abstinence Scoring System is the near commonly used scoring tool, although the original tool has been modified frequently.[v] Below is a modified Finnegan NAS Scoring grade developed by Jansson, Velez, and Harrow[iii] and farther modified by the Fletcher Allan Hospital of Vermont. Meet Appendix A for an explanation of the scoring.
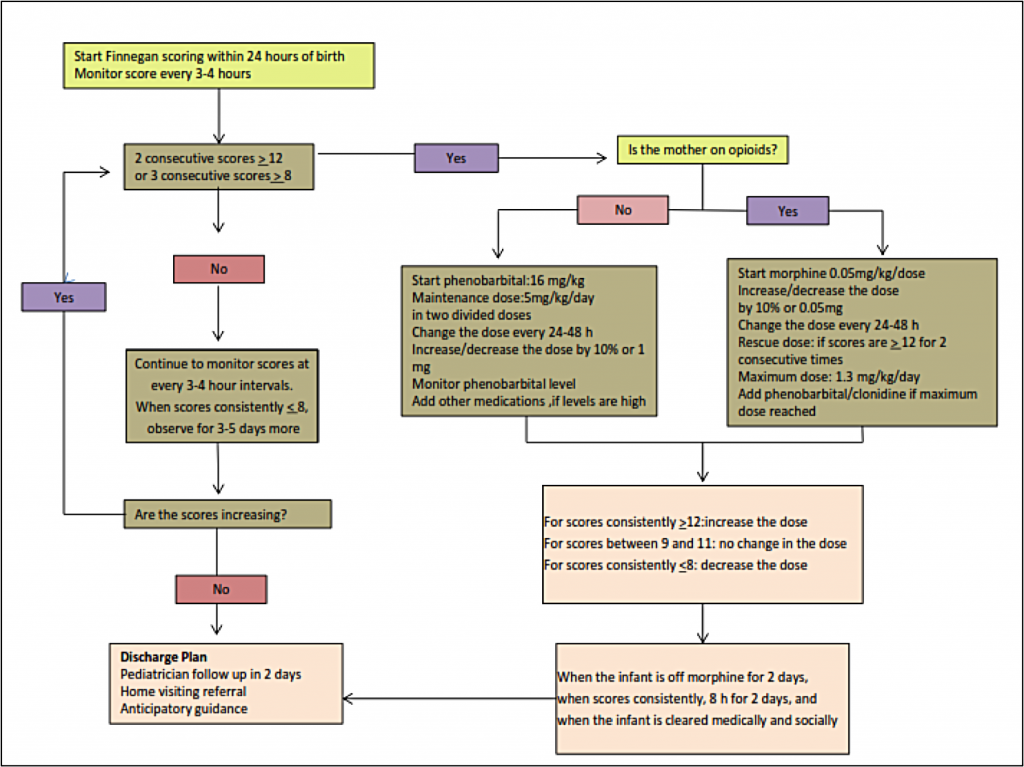
Treatment of NAS
Approximately 50% –75% of infants exposed to opioids before nascence volition require pharmacologic treatment for opioid withdrawal. At the delivery of a known opioid-dependent woman, naloxone should be avoided in resuscitation of the babe because the drug tin can precipitate seizures.
Initial treatment of infants showing signs of withdrawal is focused on supportive care. It is of import that this treatment approach is standardized inside care settings. Supportive care can include creating a low-stimulation environment that is dark and quiet, swaddling the infant to inhibit self-stimulation, and providing frequent/on-demand feedings to reduce infant stress.[i] Other beneficial strategies include encouraging skin-to-skin contact for comfort and promotion of the babe's attachment to the mother/caregiver, also every bit other comforting techniques such every bit rocking or swaying the infant.[seven] Providing frequent feedings helps to address the infant's hydration level, although many infants will require intravenous fluids to maintain adequate hydration. Frequent feedings also address the high energy expenditures associated with withdrawal (thus a need for increased calorie intake) and a symptom of withdrawal where infants engage in excessive sucking simply with poor feeding.[eight] Education these techniques to families and caregivers, including careful, detailed demonstrations, is an important gene in the success of the supportive care approach.
Breastfeeding is encouraged in cases when the female parent is receiving medication-assisted treatment and has no contraindications, such as positive HIV condition. However, the infant's weight must be advisedly monitored to ensure that the infant continues to gain weight. Breastfeeding has been associated with specific benefits for opioid-exposed infants, including less severe NAS and reduced demand for pharmacologic intervention. [ix],[ten],[11]
Pharmacologic therapy is indicated for infants who accept greater severity of symptoms of exposure and in cases in which the infant has severe airsickness, diarrhea, or excessive weight loss. Infants may be treated with a variety of medications including short-acting opioids (e.g., morphine sulfate) or long-acting opioids (due east.thou., methadone).[1] The majority of physicians in the United States use morphine or methadone in the treatment of NAS:[4]
…each nursery should develop and adhere to a standardized plan for the evaluation and comprehensive treatment of infants at risk for or showing signs of withdrawal. [i]
The Perinatal Quality Collaborative of North Carolina (PQCNC) began a quality improvement projection in 2014 for NAS. Across the land, 29 hospitals have enrolled in the quality improvement effort. The project'southward primary aim is to help hospitals provide a standardized, multidisciplinary approach to the identification, evaluation, treatment, and discharge of infants who accept experienced NAS. This protocol includes the infants' families. Each hospital squad has engaged in an intensive process of Plan, Exercise, Study, Act, to make up one's mind the most constructive standardized practices for their respective setting. The early on, important outcomes of the PQCNC endeavour to standardize NAS protocols accept included reducing the length of stay in the hospital for the infant and family unit. For more data: http://www.pqcnc.org/node/13348
Location of Care Is Specific to the Infirmary
The majority of hospitals that monitor infants for signs and symptoms of withdrawal bear such assessment on the following units:
- Female parent/Baby
- Newborn Plant nursery
- Neonatal Intensive Care Unit of measurement (NICU)
- Special Care Nursery or Level 2 nursery
- Pediatric ward
If a commitment hospital does non accept a NICU or is otherwise not equipped to provide pharmacologic treatment to the babe, the infant should be transferred to a hospital that is able to provide appropriate treatment for the infant.
Belch Considerations
A new mother undergoes meaning stress during the mail-partum period, and this stress may be heightened for a adult female who has an opioid-use disorder or is in recovery from an opioid-utilise disorder. Therefore, it is essential for the well-being of the mother and infant that a comprehensive discharge program is developed to address critical factors, including maternal substance-use disorder treatment, a rubber living surroundings, and parenting and community support. In addition, if not already involved, the mother should receive referrals to Care Coordination for Children (CC4C) and the local home-visiting program. See "Services for Women with Opioid Exposed Pregnancies in North Carolina" referral agencies.
Anticipatory Guidance
Caregivers of infants and children exposed to substances (e.g., opioids, alcohol) during their fetal development, volition demand to be enlightened of developmental milestones and track which milestones the child has achieved and those that may be lagging behind. Making the child's pediatrician enlightened of all exposures will help him or her in tracking the kid's development, including behavioral development. Referrals to specialists, including developmental-behavioral pediatricians, tin can help identify and assess other areas in which the child may need back up. Areas of focus for the pediatrician with the infant will include:
- motor deficits and cognitive delays;
- hyperactivity, impulsivity, and attention-deficit in preschool-aged children, and in addition to schoolhouse absence, schoolhouse failure, and other behavioral problems in school-anile children; and
- growth and nutritional benchmarks to identify failure to thrive and brusque stature.[6]
Caregivers of infants should give special attention to safe sleep practices (e.g., placing baby on back, removing toys, blankets, and pillows from cribs) and the elevated risk of Sudden Infant Death Syndrome (SIDS) for a substance exposed infant, should be emphasized.[12],[13],[14]
Environmental factors too have an impact on child development. Thus, an of import surface area of focus is identifying the bachelor supports and linking caregivers with those supports to promote a stable, violence free, nurturing habitation environment. The earlier a need is identified and supports are offered, the ameliorate the long-term outcomes for the child.[15]
The complexity and challenging nature of the domicile atmosphere should never be underestimated in these situations. The importance of an optimal home environs for the global evolution of these children should be emphasized to all parents. [vi]
[i] Hudak, Thou. L., Tan, R. C., Committee on Drugs, & Committee on Fetus and Newborn. (2012). Neonatal drug withdrawal. Pediatircs, 129, e540-e560. doi:10.1542/peds.2011-3212
[2] Finnegan, L.P., & Kaltenbach, K. (1992). Finnegan Neonatal Forbearance Scoring–Neonatal abstinence syndrome. In R. A. Hoekelman S.B. Friedman, Due north. G. Nelson, et al. (Eds.), Primary pediatric care ( 2d ed.; pp. 1367-1378). St. Louis, MO: Mosby.
[3] Jansson, Fifty. Thou., Velez, Chiliad., & Harrow, C. (2009). The opioid exposed newborn: Assessment and pharmacologic management. Periodical of Opioid Management, 5(i), 47-55. Retrieved from http://world wide web.ncbi.nlm.nih.gov/pmc/articles/PMC2729086/
[4] Finnegan, L. (2013). Licit and illicit drug use during pregnancy: Maternal, neonatal and early childhood consequences. (Substance Abuse in Canada Serial). Ottawa, ON: Canadian Centre on Substance Abuse. Retrieved from http://www.ccsa.ca/Eng/topics/Substance-Corruption-in-Canada/Pages/default.aspx
[5] Sarkar, S., & Donn, South. (2006). Management of neonatal abstinence syndrome in neonatal intensive care units: A national survey. Journal of Perinatology, 26, 15–17. doi:ten.1038/sj.jp.7211427
[half dozen] Kocherlakota,P. (2014). Neonatal abstinence syndrome. Pediatrics, 134, e547–e56. doi:10.1542/peds.2013-3524
[8] Sublett, J. (2013). Neonatal Abstinence Syndrome therapeutic interventions. American Periodical of Maternal/Kid Nursing, 38(2), 102-107. doi:10.1097/NMC.0b013e31826e978e
[9] Abdel-Latif, M. E., Pinner, J., Clews, S., Cooke, F., Lui, K., & Oei, J. (2006). Effects of breast milk on the severity and outcome of neonatal abstinence syndrome amongst infants of drug dependent mothers. Pediatrics, 117, e1163 -e1169. doi: 10.1542/peds.2005-1561
[10] Isemann, B., Meinzen-Derr, J., & Akinbi, H. (2011). Maternal and neonatal factors impacting response to methadone therapy in infants treated for neonatal abstinence syndrome. Journal of Perinatology, 31(1), 25–29. doi:ten.1038/jp.2010.66
[11] O'Connor, A.B., Collett, A., Alto, W. A., & O'Brien, L. Thou. (2013). Breastfeeding rates and the relationship betwixt breastfeeding and neonatal abstinence syndrome in women maintained on buprenorphine during pregnancy. Journal of Midwifery Women's Health, 58(4),383-388. doi:10.1111/jmwh.12009
[12] U.S. Department of Health and Man Services. (2006). The health consequences of involuntary exposure to tobacco smoke: A report of the Surgeon General. Atlanta, GA. Retrieved from http://www.surgeongeneral.gov/library/reports/
[thirteen] U.Due south. Department of Health and Human Services. (2014). The health consequences of smoking—50 years of progress: A report of the Surgeon General . Atlanta, GA. Retrieved from http://world wide web.surgeongeneral.gov/library/reports/
[fourteen] OLeary, C., Jacoby, P., et al. (2012). Maternal booze utilize and sudden infant death syndrome and infant mortality excluding SIDS. Pediatrics.131, e770-e778. doi:x.1542/peds.2012-1907
[xv] Hebbeler, K., Spiker, D., et al. (2007). Early intervention for infants and toddlers with disabilities and their families: Participants, services and outcomes. Final study of the National Early Intervention Longitudinal Study. U.S. Section of Education, Role of Special Education Programs.
Source: https://ncpoep.org/guidance-document/neonatal-abstinence-syndrome-overview/neonatal-abstinence-syndrome-nas/
0 Response to "How to Support a Baby Detoxing From Opiod"
Postar um comentário